 |
Editorial
Need for good quality imaging
1 Dental Institute at Guy’s King’s College and St Thomas’ Hospitals, United Kingdom
Address correspondence to:
Fraser Mc- Donald
PhD MSc BDS FDSRCS FFDRCSI FIBiol CBiol, 22nd Floor, Guy’s Tower, London SE1 9RT,
United Kingdom
Message to Corresponding Author
Article ID: 100027Z07ST2018
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Toms S, McArdle L, Brown J, McDonald F. Need for good quality imaging. J Case Rep Images Dent 2018;4:100027Z07ST2018.ABSTRACT
No Abstract
Keywords: Adenomatoid tumor, Cyst, Imaging, Unerupted bicuspid
Many countries express concern regarding the dosage of radiation associated with diagnostic imaging [1],[2]. When analysing prescription data to support guideline development, publications often recognise the paucity of data to definitively direct clinical practice.
Recent advances in imaging technology have identified the improved quality of imaging but concerns are expressed about the increased dose of radiation and potential long term harm to the patients. The many protocols for Computed Cone Beam Tomography ranged from 13 to 769 μSv for large or medium Field of Views and 7–521 μSv for small Fields of Views [3].
Clearly many strategies are being engaged in to prevent clinical ‘screening’ using radiographs and the indiscriminate use of radiographs, often undertaken for financial gain but without consideration of the patient’s welfare, cannot be condoned.
Yet there has to be a balance when concerns and caution regarding radiation risks, resulting in a failure to produce a radiographic exposure, may lead on to inaccurate diagnoses placing the patient at risk.
Recent publications have reviewed the current status of reporting of incidental findings. In one report nearly two hundred small volume Cone Beam Computed Tomographs were reviewed and 340 incidental findings were identified. Of these only one was a major issue whilst nearly thirty percent of them required follow up [4]. This case clearly demonstrates concerns of diagnosis following radiographic follow up.
The case of a fifteen year old Afro-Caribbean patient is discussed who attended with an unerupted first premolar/ bicuspid on the left side of the maxilla. The patient had an orthodontic Angles Class I occlusion and there was no evidence of caries and facial asymmetry. There were no other signs or symptoms observed in the affected area other than the tooth was unerupted.
A rotational tomograph (Figure 1) showed a unilocular radiolucent area associated with the unerupted first premolar/bicuspid. The extent of the lesion seemed to commence from the cervical region of the first bicuspid. The lesion seemed large but did not seem to affect adjacent dental structures. There did not appear to be any involvement of the maxillary antrum.
Four experienced clinicians identified the lesion as a probable dentigerous cyst associated with the unerupted maxillary first bicuspid tooth.
Issues to be considered on reflection
When discussing the site of lesion if the current literature is reviewed, the commonest frequency of dentigerous cysts is associated with mandibular third molars, maxillary third molars, mandibular and maxillary cuspids [5],[6]. Clearly, the first premolar/bicuspid site in the maxilla is extremely rare.
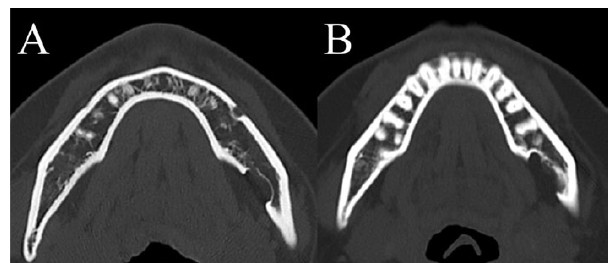
Secondly, reviewing the radiolucency on the initial dental pantomograph shows the connection of the apparent cyst is not at the cervical region but approximately 3 mm distance to the cervical cementalenamel junction. In addition, there appears to be calcified spicules/radiographic artefacts within the radiolucency (Figure 2). The appearance of the radiolucency in the maxillary first bicuspid region is unusual for dentigerous cysts.
The treatment for dentigerous cysts varies between marsupialisation and enucleation [6],[7].
The success of enucleation is significant.In order to establish the extent of the ‘cyst’ a Cone Beam Computed Tomograph was taken. However, the image produced from the CBCT showed clearly identifiable calcified spicules. As a consequence, the radiological report was changed to possible tumour. The treatment plan was then enucleation. In addition, the presence of the unerupted first bicuspid meant that the tooth would be exposed and bonded in order to allow extrusion of the unerupted tooth.The tooth was operated upon and the tissue sent for histological analysis. A section is shown with tissue supportive of the diagnosis of adenomatoid odontogenic tumour. This is not the first occasion that a cyst was actually a tumour when operated upon [8]. The treatment of this lesion was a complete enucleation. The unerupted bicuspid was exposed and a chain applied to apply traction. A subsequent radiograph showed bony infill. Treatment was uneventful. Clinically the tooth was aligned. The periodontium was sound when probed.


Conclusion
The case illustrates the use of advanced imaging to ensure an accurate diagnosis. Clinicians need to balance the risk due to radiographic exposure against the need for supportive imaging.
REFERENCE
1.
Isaacson KG, Thom AR, Atack NE, Horner K, Whaites E. Guidelines for the Use of Radiographs in Clinical Orthodontics. 4ed. London: British Orthodontic Society; 2015.

2.
Horner K, Eaton K. Selection Criteria for Dental Radiography. London: Faculty of General Dental Practitioners; 2018.
3.
Roberts JA, Drage NA, Davies J, Thomas DW. Effective dose from cone beam CT examinations in dentistry. Br J Radiol 2009 Jan;82(973):35–40. [CrossRef]
[Pubmed]
4.
Dogramaci EJ, Rossi-Fedele G, McDonald F. Clinical importance of incidental findings reported on small-volume dental cone beam computed tomography scans focused on impacted maxillary canine teeth. Oral Surg Oral Med Oral Pathol Oral Radiol 2014 Dec;118(6):e205–9. [CrossRef]
[Pubmed]
5.
Benn A, Altini M. Dentigerous cysts of inflammatory origin. A clinicopathologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996 Feb;81(2):203–9. [CrossRef]
[Pubmed]
6.
Scully C. Odontogenic cysts and tumours. Oral and Maxillofacial Medicine: The Basis of Diagnosis and Treatment. 3ed. London, UK: Churchill Livingstone Elsevier; 2013.
7.
Hyomoto M, Kawakami M, Inoue M, Kirita T. Clinical conditions for eruption of maxillary canines and mandibular premolars associated with dentigerous cysts. Am J Orthod Dentofacial Orthop 2003 Nov;124(5):515–20. [CrossRef]
[Pubmed]
8.
Sadeghi EM, Sewall SR, Dohse A, Novak TS. Odontogenic tumors that mimic a dentigerous cyst. Compend Contin Educ Dent 1995 May;16(5):500, 502, 504 passim.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Simon Toms - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Louis McArdle - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Jackie Brown - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Fraser Mc- Donald - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Revising it critically for important intellectual content, Final approval of the version to be published
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this study.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2018 Simon Toms name et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}