 |
Case Report
A case report of progressive static bone cavity in young female with endovascular intervention against the submental artery
1 MD, Director, Department of Neurosurgery, Hokuto Hospital, Obihiro, Hokkaido, Japan
Address correspondence to:
Akira Tempaku
7-5, Inada-cho-kisen, Obihiro, Hokkaido 080-0833,
Japan
Message to Corresponding Author
Article ID: 100051Z07AT2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Tempaku A. A case report of progressive static bone cavity in young female with endovascular intervention against the submental artery. J Case Rep Images Dent 2026;12(1):1–5.ABSTRACT
Introduction: Static bone cavity (SBC) is a rare, unilateral, oval-shaped radiolucent bone defect that is presumed to develop as a result of focal pressure from surrounding soft tissues. It is commonly observed in the posterior mandibular angle of adult males. It is usually asymptomatic without clinical intervention.
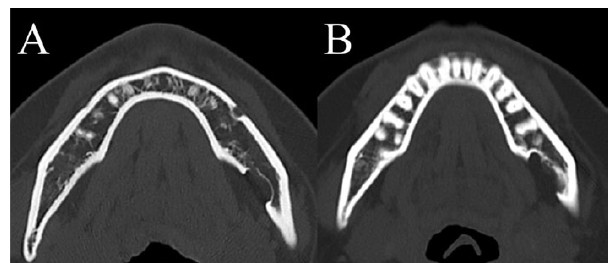
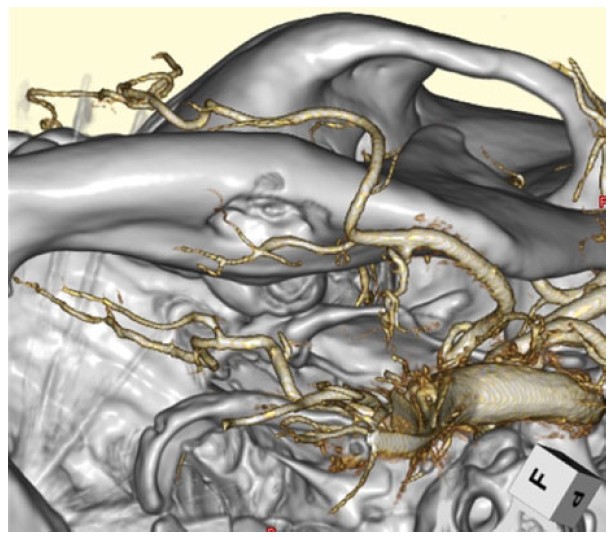
Case Report: A 36-year-old female diagnosed SBC for 10 years ago, accidentally by radiographic study. The cavity of bone defect has been enlarged gradually without any symptoms. Computed tomography (CT) showed the oval-shaped depression 20 mm × 13 mm × 8 mm in size at the left mandibular area. Magnetic resonance imaging (MRI) showed no tumor-like components in the cavity. Computed tomography angiography revealed the submental artery from the facial artery runs around the cavity. These radiographical findings presumed that localized pulsative pressure by the submental artery had formed SBC. Because of progressive enlargement of bone cavity in young female, it was afraid that mandibular bone fracture would be brought in later. To prevent the increment of bone deficit, the endovascular intervention had been performed. The submental artery was embolized by glue. Then, the growth of SBC has been suppressed after the endovascular intervention.
Conclusion: The incidence of SBC in young female is rare. Further the increment of bone deficit is observed in last 10 years without clinical deficits.
Keywords: Endovascular embolization, Static bone cavity, Submental artery, Young female
Introduction
Static bone cavity was described by Stafne as a pathological defect on the lingual mandibular bone filled with salivary gland tissues in 1941 [1],[2]. The condition was generally referred to as an asymptomatic developmental disorder detected behind the mandible of men between ages 50 and 70 [3],[4],[5],[6]. The frequency of onset has been reported to be 0.1% to 0.48% [7],[8].
Asymptomatic bone deficit in young female had been increased for last 10 years. Preventing the submandibular bone fracture in middle to elderly age time, surgical intervention was considered.
Case Report
A 36-year-old female was consulted from oral and maxillofacial surgeon. An asymptomatic static bone cavity (SBC) in the submandibular region was identified on computed tomography (CT) imaging of the face and mandible 10 years ago (Figure 1A). No abnormalities in oral function or neurological findings were noted. However, follow-up CT imaging over time revealed enlargement of the bone defect (Figure 1B). Head magnetic resonance imaging (MRI) showed no involvement of soft tissues, such as glandular tissue or muscles: T1 low, T2 low (data not shown). Head angiography revealed a submental artery branching from the facial artery, coursing around the inferior border of the mandible (Figure 2). It corresponded to the outer edge of the SBC. Located at the periphery of the bone defect site, it was thought to be the cause of bone degeneration. Bone deficit had been progressing since youth.
The cross-sectional area of the mandible bone was analyzed on CT images with axial and coronal figures. Lesion including cross-section means 19.5 mm × 16.7 mm, it showed a defect measuring 8.0 mm × 6.3 mm. Therefore, it was assessed as a 15.5% bone defect in area.
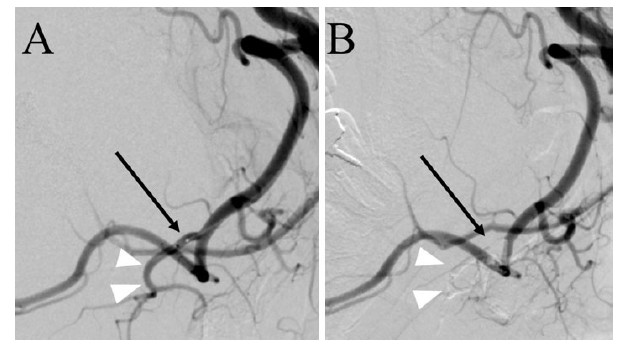
This raised concerns about the potential for mandibular fractures in the future. To prevent the progression of bone deficit, it was considered to block the pulsative pressure from a submental artery. For that reason, the submental artery occlusion by the endovascular intervention was performed. Using right femoral artery approach, a microcatheter (Defrictor Nano: Medico’s Hirata, Osaka, Japan) was guided from the left external carotid artery to the facial artery and submental artery. Endovascular occlusion glue of n-butyl-2-cyanoacrylate (NBCA) was injected from a microcatheter at a concentration of 33%. Disappearance of blood flow in the submental artery was confirmed (Figure 3).
One-year follow-up imaging showed no enlargement of the SBC (bone deficit lesion dimensions remained stable at 20 × 13 × 8 mm). No adverse events relating to the endovascular intervention were observed during the follow-up period.
The author obtained the written informed consent from the patient for the publication of this report, including images. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional committee in Hokuto hospital and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Discussion
Static bone cavity was identified in a young female patient. Although commonly seen in middle-aged men, this was a rare case, with a young age at onset and diagnosis. Generally, an asymptomatic lesion, this case was also incidentally detected on imaging. While debate exists regarding whether it is progressive or non-progressive, this case demonstrated progressive bone lesions over a period of 10 years. Serial CT scans showed enlargement of the bone defect area. Additionally, head MRI revealed no soft tissue entrapment, such as glandular tissue or fat, within the depressed area. The artery near the lesion was considered the responsible vessel.
The enlargement of the cortical bone defect area from a young age suggested a future risk of mandibular fracture complications. Therefore, treatment was deemed indicated. Traditionally, this condition was considered asymptomatic and did not require treatment intervention. However, compared to patients in middle age and older, younger individuals require securing long-term good outcomes in daily and social life. In cases of progressive lesions, the average duration of illness is longer, making early treatment intervention reasonable.
Previous literatures described four types of SBC, including posterior lingual, anterior lingual, buccal aspect of ascending ramus, and lingual aspect of ascending ramus. The posterior lingual variant is most frequently observed in submandibular gland fossa, with an incidence between 0.10% and 0.48%. The anterior lingual variant situates between the mandibular incisor and premolar area, above the insertion of mylohyoid muscle in rarely. The buccal or lingual variant is unusually located on the ascending ramus [9],[10],[11].
The cause and pathogenesis of SBC are still under discussion. Many hypotheses are proposed, such as the mandible bone forming around the submandibular salivary gland during embryonic development; insufficient bone production; abnormal vascular pressure from the facial artery causing necrotic change; and adjacent bone resorption. The most commonly accepted theory is that SBC starts from the pressure of glandular tissue on the mandible’s lingual cortex [6],[11],[12],[13]. The submandibular gland is linked to the posterior variant, while the sublingual gland is linked to the anterior variant, and the parotid gland is linked to both variants of the ascending ramus of the mandible. The bone defect is either empty or contains salivary grand, adipose, connective tissue, muscular, blood vessel or, rarely, lymph nodes [2],[6],[9],[12],[13],[14],[15],[16],[17]. In the present case, the lesion was located in the anterior lingual region, without any other tissue components. The submental artery, branched from facial artery, has been surrounded the bone edge of SBC observed. The arterial pulsatile pressure has been presumed to cause the SBC formation.
The submental artery branches off from the facial artery and supplies blood to the chin region from the inner side of the mandible. Occlusion within this branch is generally not problematic, whereas occlusion of the facial artery itself may cause taste disorders or sensory disturbances in the tip of the tongue. Therefore, during endovascular embolization, it was necessary to reliably guide the microcatheter to the submental artery and occlude that vessel. The submental artery supplies blood to the mental region, along the mandibular midline. Combined with blood flow from the contralateral side, it perfuses the tissue, making the risk of major complications from unilateral embolization relatively low.
There are also case reports of SBC caused by vascular factors [18]. It was thought that pulsatile compression from the artery, transmitted through the soft tissue between the bone and vessel, gradually eroded the mandible.
SBC is usually asymptomatic and is observed commonly in males than females with a ratio of 6:1 [2],[6],[12]. Almost all SBC cases are after the age of 40 years except one case [19]. The present case is also much rare generation in onset. Further, main cause of SBC formation is assumed not any gland tissue but submental artery. In addition, SBC location is anterior mandibular portion, where is not the most common area. This case is a rare occurrence in which several uncommon conditions overlapped as SBC.
This case report includes some limitations, such as the short follow-up duration, lack of long-term outcome data, and absence of biomechanical stress analysis against the bone fracture risk with SBC. The author needs to the long-time follow-up of radiographical change and clinical events. The fracture risk by decreased bone structure should be analyzed by biomechanical characters with mathematical methods in future.
Conclusion
A young female patient presented with progressive SBC. Pulsatile pressure originating from the submental artery was suspected to be the cause. Selective vascular embolization was performed to prevent future mandibular fracture. Post-endovascular intervention, there has been no enlargement of the bone defect.
REFERENCE
1.
Hisatomi M, Munhoz L, Asaumi J, Arita ES. Stafne bone defects radiographic features in panoramic radiographs: Assessment of 91 cases. Med Oral Patol Oral Cir Bucal 2019;24(1):e12–9. [CrossRef]
[Pubmed]

2.
Stafne EC. Bone cavities situated near the angle of the mandible. The Journal of the American Dental Association 1942;29(17):1969–72. [CrossRef]
3.
Philipsen HP, Takata T, Reichart PA, Sato S, Suei Y. Lingual and buccal mandibular bone depressions: A review based on 583 cases from a world-wide literature survey, including 69 new cases from Japan. Dentomaxillofac Radiol 2002;31(5):281–90. [CrossRef]
[Pubmed]
4.
Liang J, Deng Z, Gao H. Stafne’s bone defect: A case report and review of literatures. Ann Transl Med 2019;7(16):399. [CrossRef]
[Pubmed]
5.
Minowa K, Inoue N, Sawamura T, Matsuda A, Totsuka Y, Nakamura M. Evaluation of static bone cavities with CT and MRI. Dentomaxillofac Radiol 2003;32(1):2–7. [CrossRef]
[Pubmed]
6.
Sisman Y, Miloglu O, Sekerci AE, Yilmaz AB, Demirtas O, Tokmak TT. Radiographic evaluation on prevalence of Stafne bone defect: A study from two centres in Turkey. Dentomaxillofac Radiol 2012;41(2):152–8. [CrossRef]
[Pubmed]
7.
Assaf AT, Solaty M, Zrnc TA, Fuhrmann AW, Scheuer H, Heiland M, et al. Prevalence of Stafne’s bone cavity – Retrospective analysis of 14,005 panoramic views. In Vivo 2014;28(6):1159–64.
[Pubmed]
8.
Schneider T, Filo K, Locher MC, Gander T, Metzler P, Grätz KW, et al. Stafne bone cavities: Systematic algorithm for diagnosis derived from retrospective data over a 5-year period. Br J Oral Maxillofac Surg 2014;52(4):369–74.
[Pubmed]
9.
Etöz M, Etöz OA, Sahman H, Sekerci AE, Polat HB. An unusual case of multilocular Stafne bone cavity. Dentomaxillofac Radiol 2012;41(1):75–8. [CrossRef]
[Pubmed]
10.
Quesada-Gómez C, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Stafne bone cavity: A retrospective study of 11 cases. Med Oral Patol Oral Cir Bucal 2006;11(3):E277–80.
[Pubmed]
11.
Belmonte-Caro R, Vélez-Gutiérrez MJ, García De La Vega-Sosa FJ, García-Perla-García A, Infante-Cossío PA, Díaz-Fernández JM, et al. A Stafne’s cavity with unusual location in the mandibular anterior area. Med Oral Patol Oral Cir Bucal 2005;10(2):173–9.
[Pubmed]
12.
Dolanmaz D, Etöz OA, Pampu AA, Kılıç E, Şişman Y. Diagnosis of Stafne’s bone cavity with dental computerized tomography. Eur J Gen Med 2009;6(1):42–45. [CrossRef]
13.
Nikzad S, Azari A, Khezri F. Diagnosis of a lingual mandibular bone defect (Stafne’s bone defect) by CT Scan. Iran J Radiol 2010;7(1):27–30.
14.
Terro W, Crean J. Not all radiolucent images are pathological lesions (Stafne cyst). Dental News 2006;13(3):22–27.
15.
Branstetter BF, Weissman JL, Kaplan SB. Imaging of a Stafne bone cavity: What MR adds and why a new name is needed. AJNR Am J Neuroradiol 1999;20(4):587–9.
[Pubmed]
16.
Segev Y, Puterman M, Bodner L. Stafne bone cavity – Magnetic resonance imaging. Med Oral Patol Oral Cir Bucal 2006;11(4):E345–7.
[Pubmed]
17.
Sisman Y, Etöz OA, Mavili E, Sahman H, Tarim Ertas E. Anterior Stafne bone defect mimicking a residual cyst: A case report. Dentomaxillofac Radiol 2010;39(2):124–6. [CrossRef]
[Pubmed]
18.
Harvey W, Noble HW. Defects on the lngual surface of the mandible near the angle. Br J Oral Surg 1968;6(2):75–83. [CrossRef]
[Pubmed]
19.
Watanabe A, Yoshida S, Kato H, Matsuzaka K, Takano M. A rare case of static bone cavity in the anterior mandibular region of a 10-year-old boy. Int J Surg Case Rep 2021;83:106019. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Akira Tempaku - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
AcknowledgmentsThe author thanks medical staff of Hokuto Hospital for their support in the clinical treatment and care of the patient.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2026 Akira Tempaku. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}